

Drones are just one of several new technologies that are rising to the challenge of more frequent wildfires.
Robots have been a game-changer. Inspired by Paris, the Los Angeles Fire Department (LAFD) was the first in the U.S. to deploy a firefighting robot in 2021, the Thermite Robotics System 3 – RS3, for short.
RS3 is a 3,500-pound turbine on a crawler—the size of a Smart car—with a 36.8 horsepower engine that can go for 20 hours without refueling. It can plow through hazardous terrain, move cars from its path, and pull an 8,000-pound object from a fire.
All that while spurting 2,500 gallons of water per minute with a rear exhaust fan clearing the smoke. At a recent trade show, RS3 was billed as equivalent to 10 firefighters. The Los Angeles Times referred to it as “a droid on steroids.”

Robots such as the Thermite RS3 can plow through hazardous terrain and pull an 8,000-pound object from a fire.
Los Angeles Fire Department
The advantage of the robot is obvious. Operated remotely from a distance, it greatly reduces an emergency responder’s exposure to danger, says Wade White, assistant chief of the LAFD. The robot can be sent into airplane fires, nuclear reactors, hazardous areas with carcinogens (think East Palestine, Ohio), or buildings where a roof collapse is imminent.
Advances for firefighters are taking many other forms as well. Fibers have been developed that make the firefighter’s coat lighter and more protective from carcinogens. New wearable devices track firefighters’ biometrics in real time so commanders can monitor their heat stress and exertion levels. A sensor patch is in development which takes readings every four seconds to detect dangerous gases such as methane and carbon dioxide. A sonic fire extinguisher is being explored that uses low frequency soundwaves to remove oxygen from air molecules without unhealthy chemical compounds.
The demand for this technology is only increasing, especially with the recent rise in wildfires. In 2021, fires were responsible for 3,800 deaths and 14,700 injuries of civilians in this country. Last year, 68,988 wildfires burned down 7.6 million acres. Whether the next generation of firefighting can address these new challenges could depend on special cameras, robots of the aerial variety, AI and smart systems.
Fighting fire with cameras
Another key innovation for firefighters is a thermal imaging camera (TIC) that improves visibility through smoke. “At a fire, you might not see your hand in front of your face,” says White. “Using the TIC screen, you can find the door to get out safely or see a victim in the corner.” Since these cameras were introduced in the 1990s, the price has come down enough (from $10,000 or more to about $700) that every LAFD firefighter on duty has been carrying one since 2019, says White.
TICs are about the size of a cell phone. The camera can sense movement and body heat so it is ideal as a search tool for people trapped in buildings. If a firefighter has not moved in 30 seconds, the motion detector picks that up, too, and broadcasts a distress signal and directional information to others.
To enable firefighters to operate the camera hands-free, the newest TICs can attach inside a helmet. The firefighter sees the images inside their mask.
TICs also can be mounted on drones to get a bird’s-eye, 360 degree view of a disaster or scout for hot spots through the smoke. In addition, the camera can take photos to aid arson investigations or help determine the cause of a fire.
More help From above
Firefighters prefer the term “unmanned aerial systems” (UAS) to drones to differentiate them from military use.
A UAS carrying a camera can provide aerial scene monitoring and topography maps to help fire captains deploy resources more efficiently. At night, floodlights from the drone can illuminate the landscape for firefighters. They can drop off payloads of blankets, parachutes, life preservers or radio devices for stranded people to communicate, too. And like the robot, the UAS reduces risks for ground crews and helicopter pilots by limiting their contact with toxic fumes, hazardous chemicals, and explosive materials.
“The nice thing about drones is that they perform multiple missions at once,” says Sean Triplett, team lead of fire and aviation management, tools and technology at the Forest Service.
Experts predict we’ll see swarms of drones dropping water and fire retardant on burning buildings and forests in the near future.
The UAS is especially helpful during wildfires because it can track fires, get ahead of wind currents and warn firefighters of wind shifts in real time. The U.S. Forest Service also uses long endurance, solar-powered drones that can fly for up to 30 days at a time to detect early signs of wildfire. Wildfires are no longer seasonal in California – they are a year-long threat, notes Thanh Nguyen, fire captain at the Orange County Fire Authority.
In March, Nguyen’s crew deployed a drone to scope out a huge landslide following torrential rains in San Clemente, CA. Emergency responders used photos and videos from the drone to survey the evacuated area, enabling them to stay clear of ground on the hillside that was still sliding.
Improvements in drone batteries are enabling them to fly for longer with heavier payloads. Experts predict we’ll see swarms of drones dropping water and fire retardant on burning buildings and forests in the near future.
AI to the rescue
The biggest peril for a firefighter is often what they don’t see coming. Flashovers are a leading cause of firefighter deaths, for example. They occur when flammable materials in an enclosed area ignite almost instantaneously. Or dangerous backdrafts can happen when a firefighter opens a window or door; the air rushing in can ignite a fire without warning.
The Fire Fighting Technology Group at the National Institute of Standards and Technology (NIST) is developing tools and systems to predict these potentially lethal events with computer models and artificial intelligence.
Partnering with other institutions, NIST researchers developed the Flashover Prediction Neural Network (FlashNet) after looking at common house layouts and running sets of scenarios through a machine-learning model. In the lab, FlashNet was able to predict a flashover 30 seconds before it happened with 92.1% success. When ready for release, the technology will be bundled with sensors that are already installed in buildings, says Anthony Putorti, leader of the NIST group.
The NIST team also examined data from hundreds of backdrafts as a basis for a machine-learning model to predict them. In testing chambers the model predicted them correctly 70.8% of the time; accuracy increased to 82.4% when measures of backdrafts were taken in more positions at different heights in the chambers. Developers are working on how to integrate the AI into a small handheld device that can probe the air of a room through cracks around a door or through a created opening, Putorti says. This way, the air can be analyzed with the device to alert firefighters of any significant backdraft risk.
Early wildfire detection technologies based on AI are in the works, too. The Forest Service predicts the acreage burned each year during wildfires will more than triple in the next 80 years. By gathering information on historic fires, weather patterns, and topography, says White, AI can help firefighters manage wildfires before they grow out of control and create effective evacuation plans based on population data and fire patterns.
The future is connectivity
We are in our infancy with “smart firefighting,” says Casey Grant, executive director emeritus of the Fire Protection Research Foundation. Grant foresees a new era of cyber-physical systems for firefighters—a massive integration of wireless networks, advanced sensors, 3D simulations, and cloud services. To enhance teamwork, the system will connect all branches of emergency responders—fire, emergency medical services, law enforcement.
FirstNet (First Responder Network Authority) now provides a nationwide high-speed broadband network with 5G capabilities for first responders through a terrestrial cell network. Battling wildfires, however, the Forest Service needed an alternative because they don’t always have access to a power source. In 2022, they contracted with Aerostar for a high altitude balloon (60,000 feet up) that can extend cell phone power and LTE. “It puts a bubble of connectivity over the fire to hook in the internet,” Triplett explains.
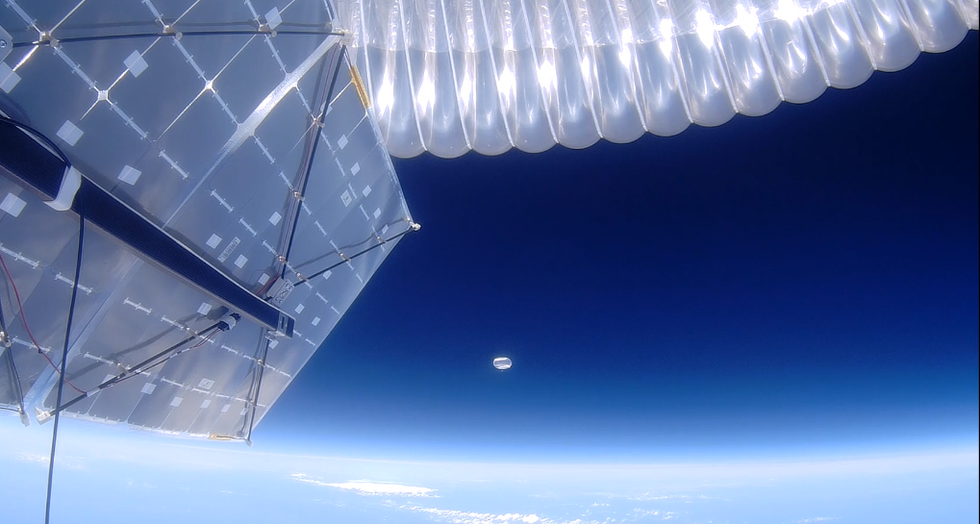
A high altitude balloon, 60,000 feet high, can extend cell phone power and LTE, putting a "bubble" of internet connectivity over fires.
Courtesy of USDA Forest Service
Advances in harvesting, processing and delivering data will improve safety and decision-making for firefighters, Grant sums up. Smart systems may eventually calculate fire flow paths and make recommendations about the best ways to navigate specific fire conditions. NIST’s plan to combine FlashNet with sensors is one example.
The biggest challenge is developing firefighting technology that can work across multiple channels—federal, state, local and tribal systems as well as for fire, police and other emergency services— in any location, says Triplett. “When there’s a wildfire, there are no political boundaries,” he says. “All hands are on deck.”

(Left to right) Vickie Naylor, Bernadine Clay, and Donna Maxey read a memory prompt as they take part in the Sharing History through Active Reminiscence and Photo-Imagery (SHARP) study, September 20, 2017.
In 2020, a first-of-its kind study in JAMA linked Alzheimer’s incidence to “neighborhood disadvantage,” which is based on SDOH indicators. Through autopsies, researchers analyzed brain tissue markers related to Alzheimer’s and found an association with these indicators. In 2022, Ryan Powell, the lead author of that study, published further findings that neighborhood disadvantage was connected with having more neurofibrillary tangles and amyloid plaques, the main pathological features of Alzheimer's disease.
As of yet, little is known about the biological processes behind this, says Powell, director of data science at the Center for Health Disparities Research at the University of Wisconsin School of Medicine and Public Health. “We know the association but not the direct causal pathway.”
The corroborative findings keep coming. In a Nature study published a few months after Powell’s study, every social determinant investigated affected Alzheimer’s risk except for marital status. The links were highest for income, education, and occupational status.
Clinical trials on new Alzheimer’s medications get all the headlines but preventing dementia through policy and public health interventions should not be underestimated.
The potential for prevention is significant. One in three older adults dies with Alzheimer's or another dementia—more than breast and prostate cancers combined. Further, a 2020 report from the Lancet Commission determined that about 40 percent of dementia cases could theoretically be prevented or delayed by managing the risk factors that people can modify.
Take inactivity. Older adults who took 9,800 steps daily were half as likely to develop dementia over the next 7 years, in a 2022 JAMA study. Hearing loss, another risk factor that can be managed, accounts for about 9 percent of dementia cases.
Clinical trials on new Alzheimer’s medications get all the headlines but preventing dementia through policy and public health interventions should not be underestimated. Simply slowing the course of Alzheimer’s or delaying its onset by five years would cut the incidence in half, according to the Global Council on Brain Health.
Minorities Hit the Hardest
The World Health Organization defines SDOH as “conditions in which people are born, work, live, and age, and the wider set of forces and systems shaping the conditions of daily life.”
Anyone who exists on processed food, smokes cigarettes, or skimps on sleep has heightened risks for dementia. But minority groups get hit harder. Older Black Americans are twice as likely to have Alzheimer’s or another form of dementia as white Americans; older Hispanics are about one and a half times more likely.
This is due in part to higher rates of diabetes, obesity, and high blood pressure within these communities. These diseases are linked to Alzheimer’s, and SDOH factors multiply the risks. Blacks and Hispanics earn less income on average than white people. This means they are more likely to live in neighborhoods with limited access to healthy food, medical care, and good schools, and suffer greater exposure to noise (which impairs hearing) and air pollution—additional risk factors for dementia.
Related Reading: The Toxic Effects of Noise and What We're Not Doing About it
Plus, when Black people are diagnosed with dementia, their cognitive impairment and neuropsychiatric symptom are more advanced than in white patients. Why? Some African-Americans delay seeing a doctor because of perceived discrimination and a sense they will not be heard, says Carl V. Hill, chief diversity, equity, and inclusion officer at the Alzheimer’s Association.
Misinformation about dementia is another issue in Black communities. The thinking is that Alzheimer’s is genetic or age-related, not realizing that diet and physical activity can improve brain health, Hill says.
African Americans are severely underrepresented in clinical trials for Alzheimer’s, too. So, researchers miss the opportunity to learn more about health disparities. “It’s a bioethical issue,” Hill says. “The people most likely to have Alzheimer’s aren’t included in the trials.”
The Cure: Systemic Change
People think of lifestyle as a choice but there are limitations, says Muniza Anum Majoka, a geriatric psychiatrist and assistant professor of psychiatry at Yale University, who published an overview of SDOH factors that impact dementia. “For a lot of people, those choices [to improve brain health] are not available,” she says. If you don’t live in a safe neighborhood, for example, walking for exercise is not an option.
Hill wants to see the focus of prevention shift from individual behavior change to ensuring everyone has access to the same resources. Advice about healthy eating only goes so far if someone lives in a food desert. Systemic change also means increasing the number of minority physicians and recruiting minorities in clinical drug trials so studies will be relevant to these communities, Hill says.
Based on SDOH impact research, raising education levels has the most potential to prevent dementia. One theory is that highly educated people have a greater brain reserve that enables them to tolerate pathological changes in the brain, thus delaying dementia, says Majoka. Being curious, learning new things and problem-solving also contribute to brain health, she adds. Plus, having more education may be associated with higher socioeconomic status, more access to accurate information and healthier lifestyle choices.
New Strategies
The chasm between what researchers know about brain health and how the knowledge is being applied is huge. “There’s an explosion of interest in this area. We’re just in the first steps,” says Powell. One day, he predicts that physicians will manage Alzheimer’s through precision medicine customized to the patient’s specific risk factors and needs.
Raina Croff, assistant professor of neurology at Oregon Health & Science University School of Medicine, created the SHARP (Sharing History through Active Reminiscence and Photo-imagery) walking program to forestall memory loss in African Americans with mild cognitive impairment or early dementia.
Participants and their caregivers walk in historically black neighborhoods three times a week over six months. A smart tablet provides information about “Memory Markers” they pass, such as the route of a civil rights march. People celebrate their community and culture while “brain health is running in the background,” Croff says.

Photos and memory prompts engage participants in the SHARP program.
OHSU/Kristyna Wentz-Graff
The project began in 2015 as a pilot study in Croff’s hometown of Portland, Ore., expanded to Seattle, and will soon start in Oakland, Calif. “Walking is good for slowing [brain] decline,” she says. A post-study assessment of 40 participants in 2017 showed that half had higher cognitive scores after the program; 78 percent had lower blood pressure; and 44 percent lost weight. Those with mild cognitive impairment showed the most gains. The walkers also reported improved mood and energy along with increased involvement in other activities.
It’s never too late to reap the benefits of working your brain and being socially engaged, Majoka says.
In Milwaukee, the Wisconsin Alzheimer’s Institute launched the The Amazing Grace Chorus® to stave off cognitive decline in seniors. People in early stages of Alzheimer’s practice and perform six concerts each year. The activity provides opportunities for social engagement, mental stimulation, and a support network. Among the benefits, 55 percent reported better communication at home and nearly half of participants said they got involved with more activities after participating in the chorus.
Private companies are offering intervention services to healthcare providers and insurers to manage SDOH, too. One such service, MyHello, makes calls to at-risk people to assess their needs—be it food, transportation or simply a friendly voice. Having a social support network is critical for seniors, says Majoka, noting there was a steep decline in cognitive function among isolated elders during Covid lockdowns.
About 1 in 9 Americans age 65 or older live with Alzheimer’s today. With a surge in people with the disease predicted, public health professionals have to think more broadly about resource targets and effective intervention points, Powell says.
Beyond breakthrough pills, that is. Like Dorothy in Kansas discovering happiness was always in her own backyard, we are beginning to learn that preventing Alzheimer’s is in our reach if only we recognized it.
This fall, Robert Reinhart of Boston University published a study finding that electrical stimulation can boost memory - and Reinhart was surprised to discover the effects lasted a full month.
Scientists believe brain circuits tend to uncouple as we age. Since brain neurons communicate by exchanging electrical impulses with each other, the breakdown of these links and associations could be what causes the “senior moment”—when you can’t remember the name of the movie you just watched.
In 2019, Boston University researchers led by Robert Reinhart, director of the Cognitive and Clinical Neuroscience Laboratory, showed that memory loss in healthy older adults is likely caused by these disconnected brain networks. When Reinhart and his team stimulated two key areas of the brain with mild electrical current, they were able to bring the brains of older adult subjects back into sync — enough so that their ability to remember small differences between two images matched that of much younger subjects for at least 50 minutes after the testing stopped.
Reinhart wowed the neuroscience community once again this fall. His newer study in Nature Neuroscience presented 150 healthy participants, ages 65 to 88, who were able to recall more words on a given list after 20 minutes of low-intensity electrical stimulation sessions over four consecutive days. This amounted to a 50 to 65 percent boost in their recall.
Even Reinhart was surprised to discover the enhanced performance of his subjects lasted a full month when they were tested again later. Those who benefited most were the participants who were the most forgetful at the start.
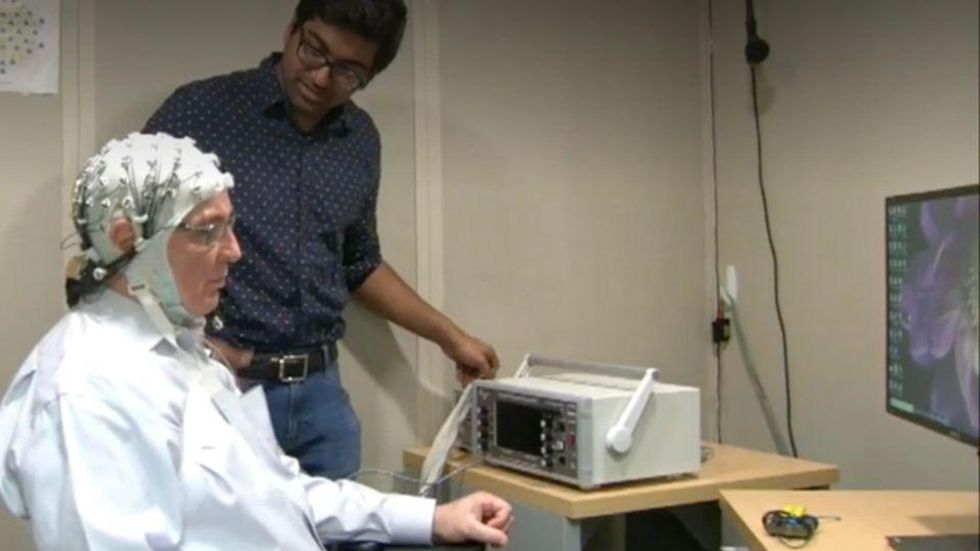
An older person participates in Robert Reinhart's research on brain stimulation.
Robert Reinhart
Reinhart’s subjects only suffered normal age-related memory deficits, but NIBS has great potential to help people with cognitive impairment and dementia, too, says Krista Lanctôt, the Bernick Chair of Geriatric Psychopharmacology at Sunnybrook Health Sciences Center in Toronto. Plus, “it is remarkably safe,” she says.
Lanctôt was the senior author on a meta-analysis of brain stimulation studies published last year on people with mild cognitive impairment or later stages of Alzheimer’s disease. The review concluded that magnetic stimulation to the brain significantly improved the research participants’ neuropsychiatric symptoms, such as apathy and depression. The stimulation also enhanced global cognition, which includes memory, attention, executive function and more.
This is the frontier of neuroscience.
The two main forms of NIBS – and many questions surrounding them
There are two types of NIBS. They differ based on whether electrical or magnetic stimulation is used to create the electric field, the type of device that delivers the electrical current and the strength of the current.
Transcranial Current Brain Stimulation (tES)is an umbrella term for a group of techniques using low-wattage electrical currents to manipulate activity in the brain. The current is delivered to the scalp or forehead via electrodes attached to a nylon elastic cap or rubber headband.
Variations include how the current is delivered—in an alternating pattern or in a constant, direct mode, for instance. Tweaking frequency, potency or target brain area can produce different effects as well. Reinhart’s 2022 study demonstrated that low or high frequencies and alternating currents were uniquely tied to either short-term or long-term memory improvements.
Sessions may be 20 minutes per day over the course of several days or two weeks. “[The subject] may feel a tingling, warming, poking or itching sensation,” says Reinhart, which typically goes away within a minute.
The other main approach to NIBS is Transcranial Magnetic Simulation (TMS). It involves the use of an electromagnetic coil that is held or placed against the forehead or scalp to activate nerve cells in the brain through short pulses. The stimulation is stronger than tES but similar to a magnetic resonance imaging (MRI) scan.
The subject may feel a slight knocking or tapping on the head during a 20-to-60-minute session. Scalp discomfort and headaches are reported by some; in very rare cases, a seizure can occur.
No head-to-head trials have been conducted yet to evaluate the differences and effectiveness between electrical and magnetic current stimulation, notes Lanctôt, who is also a professor of psychiatry and pharmacology at the University of Toronto. Although TMS was approved by the FDA in 2008 to treat major depression, both techniques are considered experimental for the purpose of cognitive enhancement.
“One attractive feature of tES is that it’s inexpensive—one-fifth the price of magnetic stimulation,” Reinhart notes.
Don’t confuse either of these procedures with the horrors of electroconvulsive therapy (ECT) in the 1950s and ‘60s. ECT is a more powerful, riskier procedure used only as a last resort in treating severe mental illness today.
Clinical studies on NIBS remain scarce. Standardized parameters and measures for testing have not been developed. The high heterogeneity among the many existing small NIBS studies makes it difficult to draw general conclusions. Few of the studies have been replicated and inconsistencies abound.
Scientists are still lacking so much fundamental knowledge about the brain and how it works, says Reinhart. “We don’t know how information is represented in the brain or how it’s carried forward in time. It’s more complex than physics.”
Lanctôt’s meta-analysis showed improvements in global cognition from delivering the magnetic form of the stimulation to people with Alzheimer’s, and this finding was replicated inan analysis in the Journal of Prevention of Alzheimer’s Disease this fall. Neither meta-analysis found clear evidence that applying the electrical currents, was helpful for Alzheimer’s subjects, but Lanctôt suggests this might be merely because the sample size for tES was smaller compared to the groups that received TMS.
At the same time, London neuroscientist Marco Sandrini, senior lecturer in psychology at the University of Roehampton, critically reviewed a series of studies on the effects of tES on episodic memory. Often declining with age, episodic memory relates to recalling a person’s own experiences from the past. Sandrini’s review concluded that delivering tES to the prefrontal or temporoparietal cortices of the brain might enhance episodic memory in older adults with Alzheimer’s disease and amnesiac mild cognitive impairment (the predementia phase of Alzheimer’s when people start to have symptoms).
Researchers readily tick off studies needed to explore, clarify and validate existing NIBS data. What is the optimal stimulus session frequency, spacing and duration? How intense should the stimulus be and where should it be targeted for what effect? How might genetics or degree of brain impairment affect responsiveness? Would adjunct medication or cognitive training boost positive results? Could administering the stimulus while someone sleeps expedite memory consolidation?
Using MRI or another brain scan along with computational modeling of the current flow, a clinician could create a treatment that is customized to each person’s brain.
While Sandrini’s review reported improvements induced by tES in the recall or recognition of words and images, there is no evidence it will translate into improvements in daily activities. This is another question that will require more research and testing, Sandrini notes.
Scientists are still lacking so much fundamental knowledge about the brain and how it works, says Reinhart. “We don’t know how information is represented in the brain or how it’s carried forward in time. It’s more complex than physics.”
Where the science is headed
Learning how to apply precision medicine to NIBS is the next focus in advancing this technology, says Shankar Tumati, a post-doctoral fellow working with Lanctôt.
There is great variability in each person’s brain anatomy—the thickness of the skull, the brain’s unique folds, the amount of cerebrospinal fluid. All of these structural differences impact how electrical or magnetic stimulation is distributed in the brain and ultimately the effects.
Using MRI or another brain scan along with computational modeling of the current flow, a clinician could create a treatment that is customized to each person’s brain, from where to put the electrodes to determining the exact dose and duration of stimulation needed to achieve lasting results, Sandrini says.
Above all, most neuroscientists say that largescale research studies over long periods of time are necessary to confirm the safety and durability of this therapy for the purpose of boosting memory. Short of that, there can be no FDA approval or medical regulation for this clinical use.
Lanctôt urges people to seek out clinical NIBS trials in their area if they want to see the science advance. “That is how we’ll find the answers,” she says, predicting it will be 5 to 10 years to develop each additional clinical application of NIBS. Ultimately, she predicts that reigning in Alzheimer’s disease and mild cognitive impairment will require a multi-pronged approach that includes lifestyle and medications, too.
Sandrini believes that scientific efforts should focus on preventing or delaying Alzheimer’s. “We need to start intervention earlier—as soon as people start to complain about forgetting things,” he says. “Changes in the brain start 10 years before [there is a problem]. Once Alzheimer’s develops, it is too late.”