
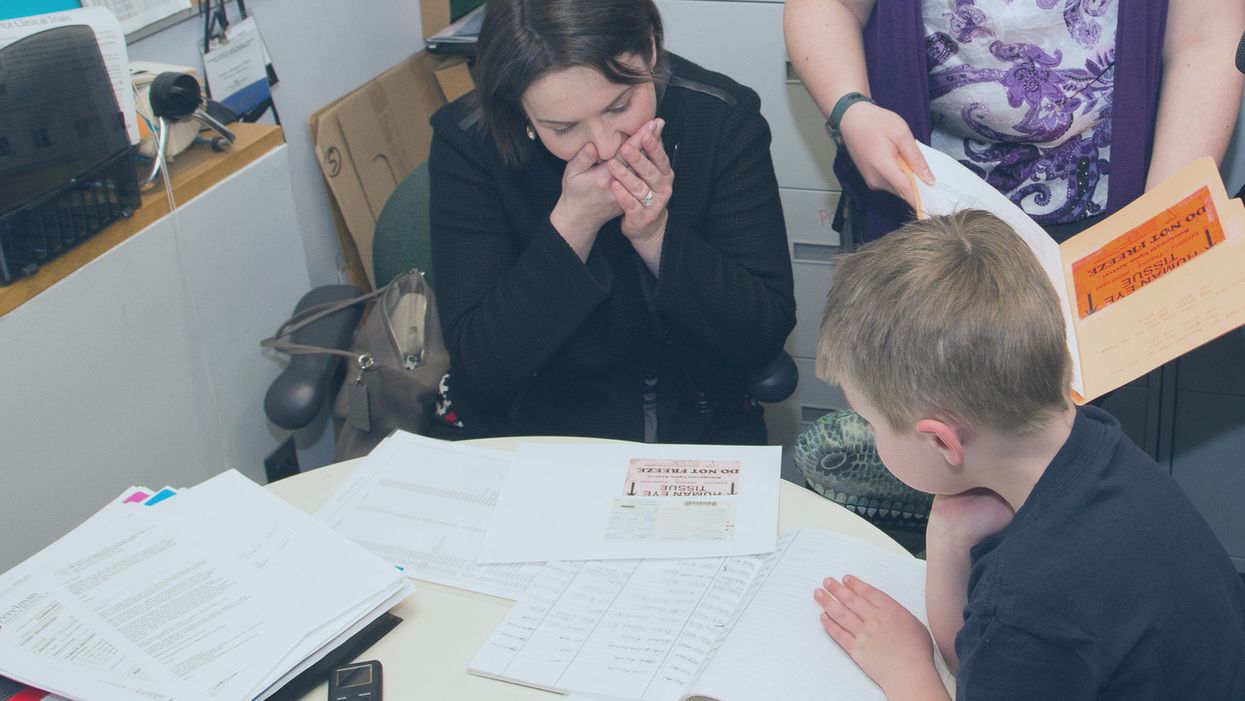
Sarah Gray views data about the use of her deceased son Thomas' retinal tissue in research for retinoblastoma, a cancer of the eye, at the University of Pennsylvania, while her son Callum looks on.
The twin boys growing within her womb filled Sarah Gray with both awe and dread. The sonogram showed that one, Callum, seemed to be the healthy child she and husband Ross had long sought; the other, Thomas, had anencephaly, a fatal developmental disorder of the skull and brain that likely would limit his life to hours. The options were to carry the boys to term or terminate both.
The decision to donate Thomas' tissue to research comforted Sarah. It brought a sense of purpose and meaning to her son's anticipated few breaths.
Sarah learned that researchers prize tissue as essential to better understanding and eventually treating the rare disorder that afflicted her son. And that other tissue from the developing infant might prove useful for transplant or basic research.
Animal models have been useful in figuring out some of the basics of genetics and how the body responds to disease. But a mouse is not a man. The new tools of precision medicine that measure gene expression, proteins and metabolites – the various chemical products and signals that fluctuate in health and illness – are most relevant when studying human tissue directly rather than in animals.
The decision to donate Thomas' tissue to research comforted Sarah. It brought a sense of purpose and meaning to her son's anticipated few breaths.

Thomas Gray
(Photo credit: Mark Walpole)
Later Sarah would track down where some of the donated tissues had been sent and how they were being used. It was a rare initiative that just may spark a new kind of relationship between donor families and researchers who use human tissue.
Organ donation for transplant gets all the attention. That process is simple, direct, life saving, the stories are easy to understand and play out regularly in the media. Reimbursement fully covers costs.
Tissue donation for research is murkier. Seldom is there a direct one-to-one correlation between individual donation and discovery; often hundreds, sometimes thousands of samples are needed to tease out the basic mechanisms of a disease, even more to develop a treatment or cure. The research process can be agonizingly slow. And somebody has to pay for collecting, processing, and getting donations into the hands of appropriate researchers. That story rarely is told, so most people are not even aware it is possible, let alone vital to research.
Gray set out on a quest to follow where Thomas' tissue had gone and how it was being used to advance research and care.
The dichotomy between transplant and research became real for Sarah several months after the birth of her twins, and Thomas' brief life, at a meeting for families of transplant donors. Many of the participants had found closure to their grieving through contact with grateful recipients of a heart, liver, or kidney who had gained a new lease on life. But there was no similar process for those who donated for research. Sarah felt a bit, well, jealous. She wanted that type of connection too.
Gray set out on a quest to follow where Thomas' tissue had gone and how it was being used to advance research and care. Those encounters were as novel for the researchers as they were for Sarah. The experience turned her into an advocate for public education and financial and operational changes to put tissue donation for research on par with donations for transplant.
Thomas' retina had been collected and processed by the National Disease Research Interchange (NDRI), a nonprofit that performs such services for researchers on a cost recovery basis with support from the National Institutes of Health. The tissue was passed on to Arupa Ganguly, who is studying retinoblastoma, a cancer of the eye, at the University of Pennsylvania.
Ganguly was surprised and apprehensive months later when NDRI emailed her saying the mother of donated tissue wanted to learn more about how the retina was being used. That was unusual because research donations generally are anonymous.
The geneticist waited a day or two, then wrote an explanation of her work and forwarded it back through NDRI. Soon the researcher and mother were talking by phone and Sarah would visit the lab. Even then, Ganguly felt very uncomfortable. "Something very bad happened to your son Thomas but it was a benefit for me, so I'm feeling very bad," she told Sarah.
"And Sarah said, Arupa, you were the only ones who wanted his retinas. If you didn't request them, they would be buried in the ground. It gives me a sense of fulfillment to know that they were of some use," Ganguly recalls. And her apprehension melted away. The two became friends and have visited several times.

Sarah Gray visits Dr. Arupa Ganguly at the University of Pennsylvania's Genetic Diagnostic Laboratory.
(Photo credit: Daniel Burke)
Reading Sarah Gray's story led Gregory Grossman to reach out to the young mother and to create Hope and Healing, a program that brings donors and researchers together. Grossman is director of research programs at Eversight, a large network of eye banks that stretches from the Midwest to the East Coast. It supplies tissue for transplant and ocular research.
"Research seems a cold and distant thing," Grossman says, "we need to educate the general public on the importance and need for tissue donations for research, which can help us better understand disease and find treatments."
"Our own internal culture needs to be shifted too," he adds. "Researchers and surgeons can forget that these are precious gifts, they're not a commodity, they're not manufactured. Without people's generosity this doesn't exist."
The initial Hope and Healing meetings between researchers and donor families have gone well and Grossman hopes to increase them to three a year with support from the Lions Club. He sees it as a crucial element in trying to reverse the decline in ocular donations even while research needs continue to grow.
What people hear about is "Tuskegee, Henrietta Lacks, they hear about the scandals, they don't hear about the good news. I would like to change that."
Since writing about her experience in the 2016 book "A Life Everlasting," Gray has come to believe that potential donor families, and even people who administer donation programs, often are unaware of the possibility of donating for research.
And roadblocks are common for those who seek to do so. Just like her, many families have had to be persistent in their quest to donate, and even educate their medical providers. But Sarah believes the internet is facilitating creation of a grassroots movement of empowered donors who are pushing procurement systems to be more responsive to their desires to donate for research. A lot of it comes through anecdote, stories, and people asking, if they have done it in Virginia, or Ohio, why can't we do it here?

Callum Gray and Dr. Arupa Ganguly hug during his family's visit to the lab.
(Photo credit: Daniel Burke)
Gray has spoken at medical and research facilities and at conferences. Some researchers are curious to have contact with the families of donors, but she believes the research system fosters the belief that "you don't want to open that can of worms." And lurking in the background may be a fear of liability issues somehow arising.
"I believe that 99 percent of what happens in research is very positive, and those stories would come out if the connections could be made," says Sarah Gray. But what they hear about is "Tuskegee, Henrietta Lacks, they hear about the scandals, they don't hear about the good news. I would like to change that."

